We need to do the first screening. Screening - what is it and why is it needed. Standards for ultrasound diagnostics I screening
To eat or not to eat? And if there is, then what? Do I need an ultrasound on the day of blood donation? Can I donate blood in the morning? What about a week after the ultrasound? What should be done before the first trimester screening? Is it necessary to take a second screening during pregnancy? And in what terms?
In our clinics, dozens of women undergo daily screenings of the 1st and 2nd trimesters: they do ultrasounds and donate blood. And when you visit a doctor or in a treatment room, the most incredible questions and opinions about these studies are voiced.
The rules for taking blood tests for screening are overgrown with myths and legends. It's time to get rid of them.
So, the myths about preparing for blood donation on biochemical screening during pregnancy(double test, quadruple test, preeclampsia risk assessment)
1. You need to take the first screening at week 12, plus or minus 5 days, and the second - no later than week 18.
This is wrong. The deadlines for screening are from 11 to 13 weeks 6 days, and the second - from 14 to 20 weeks (optimally from 16 to 18, but possibly later).
2. You can donate blood for screening only in the morning.
There are no fluctuations in the biochemical parameters of screening during the day, so there is no need to specifically take it in the morning. The main thing is not earlier than 3-4 hours after the last meal (do not eat fatty foods).
3. Before each screening, you need to undergo an ultrasound scan.
Ultrasound screening of the 1st trimester is done before donating blood for a double test, and the next ultrasound is already from 19 to 21 weeks, when the screening of the second trimester (quadruple test) has already been passed. First-trimester ultrasonography with TST and nasal bones is included in the risk calculation in both screenings.
Incorrect recommendations on one of the sites:
"Blood should not be donated immediately after an ultrasound." In the case of screening, most women donate blood immediately after the first ultrasound, so as not to go to the clinic twice.
4. Before donating blood, you must follow a diet for several days with the exception of highly allergenic foods, including citrus fruits, chocolate and red fruits and vegetables. Other recommendations forbid drinking sweet soda and eating refreshing lozenges on the day of the test.
We see no reason to deny ourselves these foods in preparation for screening.
6. Cancel all medications 3 days before the test.
Only a doctor can cancel medicines during pregnancy. You do not need to do this before donating blood for screening! But to indicate the medications taken is very important for a correct assessment of the results.
7. Don't donate blood for screening if you're nervous or have a cold.
Also a myth. But we still wish you a calm, easy and healthy pregnancy!
8. You can donate blood only on the day of the ultrasound.
No, that's not true either. It is important to do an ultrasound and donate blood within the specified screening range. We recommend donating blood after performing an ultrasound scan, since ultrasound determines the period and adequacy of the development of pregnancy, and also determines the indicators that are important for the calculation.
10. If the first screening is good, the second screening is not needed.
This is wrong. The second screening complements the first, including by identifying other conditions that are not detected in the first screening.
11. If the ultrasound is good, you do not need to donate blood.
Ultrasound of the first trimester does not reveal 100% of chromosomal abnormalities, some conditions may not yet be visible. A blood test can determine a pathology that is not yet visible on an ultrasound.
So,
treat recommendations with common sense. For example, among other recommendations before screening on one site, we even found this: "Before taking blood, it is advisable to exclude the use of ... oral contraceptives." It is clear that these are just general rules that are copied to all analyzes. There were also recommendations about fasting for at least 12 hours.
Before screening, continue to lead a normal lifestyle, eat as usual, do not come up with a low-allergenic non-red diet, continue to exercise for pregnant women.
On the day of the screening, you can also eat and drink. You should not eat within 3-4 hours immediately before the test, and also eat fatty foods. No, this will not affect the result of the analysis, but in some cases it may require a retake.
The most important thing about preparation is meet screening deadlines.
Health and easy pregnancy!
Prenatal screenings cause a lot of conflicting opinions and reviews. Someone is convinced of their necessity, others are sure of their complete inexpediency. What kind of studies are these, and do all pregnant women really need to undergo them?
To understand this issue, let's weigh all the pros and cons and separate the existing myths from the objective data of scientific medicine.
is a complex of studies, the main purpose of which is to identify the risk group of pregnant women with possible malformations of the child (such as: Down syndrome, Edwards syndrome, neural tube defects (anencephaly), Cornelia de Lange syndrome, Smith Lemli Opitz syndrome, triploidy, Patau syndrome ). The expectant mother is sent for prenatal screening twice during pregnancy - in the first (at 11-13 weeks) and in the second trimester (at 18-21 weeks). And, despite the fact that screenings include only two fairly proven diagnostic methods - a biochemical blood test and ultrasound, their reliability and safety still cause a lot of controversy.
Argument No. 1: Ultrasound is harmful to the baby
There is a fairly widespread opinion that ultrasound negatively affects the nervous system of the child, irritates him - during the examination, babies often try to hide from the apparatus, cover their heads with their hands. Therefore, children whose mothers regularly had ultrasound during pregnancy are more restless compared to babies whose mothers refused ultrasound diagnostics. Is it really?
According to doctors, ultrasound cannot cause any harm to the baby at all - modern equipment is absolutely safe. Therefore, official medicine insists that absolutely all pregnant women undergo ultrasound. After all, a timely diagnosis allows, firstly, to see a complete picture of the course of pregnancy, and secondly, if necessary, to correct certain problems.
An ultrasound examination is performed at least three times during pregnancy (in the first trimester at 11-13 weeks, in the second - at 18-21 and in the third - at 30-32 weeks), but if necessary, the doctor may recommend taking it more often.
Particularly important are the data obtained from the ultrasound of the first prenatal screening (at 11-13 weeks of gestation). At this time during the study:
the number of embryos in the uterus, their viability is determined;
a more accurate gestational age is set;
gross malformations are excluded;
the thickness of the collar space is determined - TVP (that is, the amount of subcutaneous fluid on the back of the child's neck is measured - normally TVP should not exceed 2.7 mm);
the presence or absence of the nasal bone is examined.
So, for example, in children with Down syndrome, the fluid content is much higher than normal, and the nasal bone is often not visualized.
Argument "against" No. 2: a biochemical blood test gives an unreliable result
Many mothers are sure that it is impossible to draw at least some reliable conclusions from one analysis - too many factors can affect the result. And, in part, they are indeed right. However, you need to take a closer look at the analysis process in order to understand on the basis of which the doctor makes a conclusion.
Biochemical analysis is carried out in order to determine the level of specific placental proteins in the blood. During first screening is being done "double test"(that is, the level of two proteins is determined):
PAPPA (“pregnancy associated plasma protein” or pregnancy-associated plasma protein A);
free beta subunit of hCG (human chorionic gonadotropin).
A change in the level of these proteins indicates the risk of the fetus having various chromosomal and some non-chromosomal disorders. However, the identification of an increased risk is not yet evidence that something is wrong with the baby. Such indicators are only an occasion for more careful monitoring of the course of pregnancy and the development of the child. As a rule, if the risk for any indicators is increased as a result of screening in the first trimester, the expectant mother is offered to wait for the second screening. In case of serious deviations from the norm, a woman is referred for a consultation with a geneticist.
Holding second screening falls on 18-21 weeks of pregnancy. This research includes "triple" or "Quad test". Everything happens in the same way as in the first trimester - the woman again takes a blood test. Only in this case, the results of the analysis are used to determine not two, but three (or, respectively, four) indicators:
free beta subunit of hCG;
alphafetoprotein;
free estriol;
in the case of the quadruple test, also inhibin A.
As in the first screening, the interpretation of the results is based on the deviation of the indicators from the average statistical norm according to certain criteria. All calculations are carried out using a special computer program, after which they are carefully analyzed by a doctor. In addition, when analyzing the results, many individual parameters are taken into account (racial origin, the presence of chronic diseases, the number of fetuses, body weight, bad habits, etc.), since these factors can affect the value of the studied indicators.
In order to obtain the most reliable screening results, the data of the studies of the first and second trimesters in the complex are necessarily correlated.
If, as a result of studies of the I and II trimester, any abnormalities in the development of the fetus are revealed, the woman may be offered to undergo a second screening or be immediately referred for a consultation with a geneticist. If necessary, he may prescribe additional tests to make a more accurate diagnosis (for example, an examination of amniotic fluid, a chorionic villus biopsy). However, due to the fact that these studies are not entirely safe and can cause various complications during pregnancy (provoke a miscarriage, the development of a group or Rh conflict, infection of the fetus, etc.), they are prescribed only in case of a high risk of pathology. However, such complications are not so common - in 1-2% of cases. And, of course, all research is done only with the consent of the expectant mother.
Thus, the first two arguments "against", from the point of view of scientific medicine, are not convincing, and rather they should be reformulated into arguments "for": Prenatal screenings are completely safe for the expectant mother and her baby, and all conclusions are made by the doctor, taking into account a whole range of individual factors..
Cons #3: “I have good genetics – I don’t need screenings”
Some mothers do not see the point in undergoing screenings - all relatives are healthy, what problems can there be? Indeed, there are separate groups of women who are primarily recommended to undergo a study to identify possible pathologies in the development of the child. These are women over 35–40 years old (because after this age the risk of developing abnormalities in a child increases several times) and expectant mothers with certain diseases (for example, diabetes mellitus). Of course, the risk group includes those mothers whose families already have children or relatives with genetic diseases. However, most doctors (and not only in Russia, but also in many countries of Europe and America) are of the opinion that all women need to undergo prenatal screenings, especially if their first pregnancy.
Cons #4: “Afraid of hearing a bad diagnosis”
This is perhaps one of the strongest arguments "against" the passage of screenings. Expectant mothers are very afraid of hearing something bad about the development of the baby. In addition, medical errors are also worrying - sometimes screenings give a false positive or false negative result. There are cases when the mother was told that the child was suspected of having Down syndrome, and subsequently a healthy baby was born. Of course, to be sure, such news greatly affects the emotional state of the mother. After the “terrible sentence” is passed, the woman spends the rest of her pregnancy in constant worries, and this is also completely unhealthy for the baby’s health.
However, do not forget that all the results of prenatal screening in no way serve to make a diagnosis. They only determine the likely risks. Therefore, even a positive screening result will not be a "sentence" to the child. This is just an excuse to get professional advice from a geneticist.
Argument "against" No. 5: Identified potential deviations in the development of the child cannot be corrected
This is true - there is no way to cure or correct chromosomal disorders. Therefore, impressionable and vulnerable mothers, as well as women who are determined to maintain an existing pregnancy under any circumstances, can only get an extra reason for worries as a result of the screenings they have passed. Perhaps, indeed, the best way out in such a situation would be to refuse research, so that the mother could calmly wait for the birth of the baby.
Another argument for
And yet, the undoubted advantage of prenatal screenings is the opportunity to get information about the development of the child at a fairly early stage of pregnancy, go for a consultation with a geneticist, and, if necessary, undergo all additional examinations. After all, having full data, the expectant mother can already quite consciously decide on the further development or termination of pregnancy.
The main argument "against": poor health of the expectant mother at the time of the study
Any, even a slight increase in body temperature, a cold (ARI, SARS), any other viral and infectious diseases, and even stress are a clear contraindication for screening. After all, each of these factors can distort the data of the analyzes. That is why, before going to donate blood, the expectant mother must be examined by a gynecologist - the doctor will assess her general condition.
To date, prenatal screenings are not strictly mandatory, but most doctors are confident in the need for these studies. The right to make a decision remains with the mother, so, having weighed all the pros and cons, each woman will make a choice - it is important for someone to control the situation and receive all possible information as early as possible, while someone is much more comfortable with only the obligatory minimum surveys, just enjoy the pregnancy and believe in the best.
magazine for parents "Raising a Child", October 2012
Some time ago, pregnant women did not even know about such a procedure as prenatal or perinatal . Now all expectant mothers undergo such a survey.
What is pregnancy screening, why is it done, and why are results so important? Answers to these and other questions of concern to many pregnant women about perinatal screening we have tried to give in this material.
In order to exclude any further misunderstanding of the information presented, before proceeding directly to the consideration of the above topics, it is worth defining some medical terms.
Prenatal screening is a special kind of such actually standard procedure as screening. Given comprehensive examination consists of ultrasound diagnostics and laboratory research, in this particular case maternal serum biochemistry. Early detection of some genetic abnormalities - this is the main task of such an analysis during pregnancy as screening.
prenatal or perinatal means prenatal, and under the term screening in medicine, it means a series of studies of a large stratum of the population, which are carried out in order to form the so-called "risk group", prone to certain diseases.
Can be universal or selective screening
.
It means that screening studies are done not only for pregnant women, but also for other categories of people, for example, children of the same age, to establish diseases characteristic of a given period of life.
With help genetic screening doctors can learn not only about problems in the development of the baby, but also respond in time to complications during which a woman may not even suspect.
Often, expectant mothers, having heard that they will have to undergo this procedure several times, begin to panic and worry in advance. However, there is nothing to be afraid of, you just need to ask the gynecologist in advance why you need screening for pregnant women, when and, most importantly, how this procedure is done.
So, let's start with what is standard screening carried out three times during the entire pregnancy, i.e. in every trimester . Recall that trimester is a period of three months.
What it is 1st trimester screening ? First, let's answer the common question about how many weeks it is. first trimester of pregnancy . In gynecology, there are only two ways to reliably determine the period during pregnancy - calendar and obstetric.
The first is based on the day of conception, and the second depends on menstrual cycle , preceding fertilization . That's why I trimester - this is the period that, according to the calendar method, begins with the first week from conception and ends with the fourteenth week.
According to the second method, I trimester
- This is 12 obstetric weeks. Moreover, in this case, the period is counted from the beginning of the last menstruation. Recently screening
not prescribed to pregnant women. 
However, now many expectant mothers themselves are interested in undergoing such an examination.
In addition, the Ministry of Health strongly recommends that examinations be ordered for all expectant mothers without exception.
True, this is done voluntarily, because. no one can force a woman to undergo any kind of analysis.
It is worth noting that there are categories of women who are simply obliged, for one reason or another, to go through screening, For example:
- pregnant women from thirty-five years and beyond;
- expectant mothers with a history of a threat spontaneous ;
- women who in the first trimester suffered infectious diseases ;
- pregnant women who, for health reasons, are forced to take medicines prohibited for their position in the early stages;
- women who had various previous pregnancies genetic abnormalities or anomalies in the development of the fetus ;
- women who have already given birth to children with any deviations or malformations in development ;
- women who have been diagnosed frozen or regressive pregnancy (cessation of fetal development);
- suffering from narcotic or women;
- pregnant women in whose family or in the family of the father of the unborn child cases of hereditary genetic abnormalities .
At what time do prenatal screening 1st trimester ? For the first screening during pregnancy, the period is set in the interval starting from 11 weeks to 13 obstetric weeks of pregnancy and 6 days. Earlier than the indicated period, it makes no sense to conduct this survey, since its results will be uninformative and absolutely useless.
The first ultrasound at the 12th week of pregnancy is done by a woman for a reason. Since this is the end of embryonic and starts fetal or fetal period of human development.
This means that the embryo turns into a fetus, i.e. there are obvious changes that speak of the development of a full-fledged living human body. As we said before, screening studies - This is a set of measures that consists of ultrasound diagnostics and biochemistry of a woman's blood.
It is important to understand that the screening ultrasound in the 1st trimester during pregnancy plays the same important role as laboratory blood tests. After all, in order for geneticists to make the right conclusions based on the results of the examination, they need to study both the results of ultrasound and the biochemistry of the patient's blood.
We talked about how many weeks the first screening is carried out, now let's move on to deciphering the results of a comprehensive study. It is really important to consider in more detail the norms established by doctors for the results of the first screening during pregnancy. Of course, only a specialist in this field who has the necessary knowledge and, most importantly, experience can give a qualified assessment of the results of the analysis.
We believe that it is advisable for any pregnant woman to know at least general information about the main indicators prenatal screening and their standard values. After all, it is common for most expectant mothers to be overly suspicious about everything related to the health of their unborn child. Therefore, they will be much more comfortable if they know in advance what to expect from the study.
Deciphering the screening of the 1st trimester by ultrasound, norms and possible deviations
All women know that during pregnancy they will have to undergo more than once an ultrasound examination (hereinafter referred to as ultrasound), which helps the doctor track the intrauterine development of the unborn child. In order to screening ultrasound gave reliable results, you need to prepare in advance for this procedure.
We are sure that the vast majority of pregnant women know how to do this procedure. However, it is not superfluous to repeat that there are two types of research - transvaginal and transabdominal . In the first case, the sensor of the device is inserted directly into the vagina, and in the second case it is in contact with the surface of the anterior abdominal wall.

There are no special preparation rules for the transvaginal type of ultrasound.
If you are going to have a transabdominal examination, then before the procedure (approximately 4 hours before the ultrasound), you should not go to the toilet “little by little”, and it is recommended to drink up to 600 ml of plain water in half an hour.
The thing is that the examination must be carried out necessarily on a liquid-filled bladder .
In order for the doctor to get a reliable result ultrasound screening, the following conditions must be met:
- the period of the examination is from 11 to 13 obstetric weeks;
- the position of the fetus should allow the specialist to carry out the necessary manipulations, otherwise mommy will have to “influence” the baby so that he rolls over;
- coccygeal-parietal size (hereinafter KTR) should not be less than 45 mm.
What is KTP during pregnancy on ultrasound
When conducting an ultrasound, a specialist without fail examines various parameters or sizes of the fetus. This information allows you to determine how well the baby is formed and whether it is developing correctly. The norms of these indicators depend on the gestational age.
If the value of one or another parameter obtained as a result of ultrasound deviates from the norm up or down, then this is considered a signal of the presence of some pathologies. Coccyx-parietal size - This is one of the most important initial indicators of the correct intrauterine development of the fetus.
The KTP value is compared with the fetal weight and gestational age. This indicator is determined by measuring the distance from the bone of the crown of the child to his tailbone. As a general rule, the higher the KTR, the longer the gestational age.

When this indicator slightly exceeds or, on the contrary, slightly less than the norm, then there is no reason to panic. It speaks only about the peculiarities of the development of this particular child.
If the CTE value deviates from the standards upwards, then this indicates the development of a large-sized fetus, i.e. presumably, the weight of the child at birth will exceed the average norms of 3-3.5 kg. In cases where the CTE is significantly less than the standard values, this may be a sign that:
- pregnancy does not develop as it should, in such cases, the doctor should carefully check the fetal heartbeat. If he died in the womb, then the woman needs urgent medical care ( curettage of the uterine cavity ) to prevent a possible health hazard ( development of infertility ) and life ( infection, bleeding );
- the body of a pregnant woman produces an insufficient amount, as a rule, which can lead to spontaneous miscarriage. In such cases, the doctor prescribes an additional examination to the patient and prescribes medications containing hormones ( , Dufston );
- mother is sick infectious diseases , including venereal;
- the fetus has genetic abnormalities. In such situations, doctors prescribe additional studies along with, which is part of the first screening analysis.
It is also worth emphasizing that there are often cases when a low CTE indicates an incorrectly established gestational age. This refers to the variant of the norm. All a woman needs in such a situation is to undergo a second ultrasound examination after a while (usually after 7-10 days).
Fetal BDP (biparietal size)
What is BDP on ultrasound during pregnancy? When conducting an ultrasound examination of the fetus in the first trimester, doctors are interested in all possible characteristics of the unborn child. Since their study gives specialists maximum information about how the intrauterine development of a little man takes place and whether everything is in order with his health.
What is it fetal BD ? First, let's decipher the medical abbreviation. BDP - This biparietal size of the fetal head , i.e. distance between walls parietal bones of the skull , in a simple way, the size of the head. This indicator is considered one of the main indicators for determining the normal development of the child.
It is important to note that BDP shows not only how well and correctly the baby is developing, but also helps doctors prepare for the upcoming delivery. Since if the size of the head of the unborn child deviates from the norm upwards, then he simply will not be able to pass through the mother's birth canal. In such cases, a planned caesarean section is prescribed.

When BDP deviates from established norms, this may indicate:
- about the presence in the fetus of pathologies incompatible with life, such as cerebral herniation or tumor ;
- about a sufficiently large size of the unborn child, if other basic parameters of the fetus are several weeks ahead of the established development standards;
- about spasmodic development, which after some time will return to normal, provided that other basic parameters of the fetus fit into the norm;
- on fetal development brain arising from the presence of infectious diseases in the mother.
The deviation of this indicator downward indicates that the baby's brain is developing incorrectly.
Collar space thickness (TVP)
Fetal TVP - what it is? Collar space fetus or size neck fold - this is a place (more precisely, an oblong formation) located between the neck and the upper skin membrane of the baby's body, in which there is an accumulation of fluid. A study of this value is carried out during screening of the first trimester of pregnancy, since it is at this time that it is possible to measure TVP for the first time, and then analyze it.
Starting from the 14th week of pregnancy, this formation gradually decreases in size and by the 16th week it practically disappears from visibility. For TVP, certain norms are also established, which are directly dependent on the gestational age.
For example, the norm collar space thickness at 12 weeks should not go beyond the range of 0.8 to 2.2 mm. Collar space thickness at 13 weeks should be in the range from 0.7 to 2.5 mm.
It is important to note that for this indicator, experts set the average minimum values, the deviation from which indicates a thinning of the collar space, which, like the expansion of the TVP, is considered an anomaly.
![]()
If this indicator does not correspond to the TVP norms indicated in the above table at 12 weeks and at other stages of pregnancy, then this result most likely indicates the presence of the following chromosomal abnormalities:
- trisomy 13 , a disease known as patau syndrome, characterized by the presence in human cells of an additional 13th chromosome;
- trisomy on chromosome 21, known to all as down syndrome , a human genetic disease in which karyotype (i.e., the complete set of chromosomes) is represented by the 47th chromosome instead of 46;
- monosomy on the X chromosome , a genomic disease named after the scientists who discovered it Shereshevsky-Turner syndrome, it is characterized by such anomalies of physical development as short stature, as well as sexual infantilism (immaturity);
- trisomy 18 is a chromosomal disorder. For Edwards syndrome (the second name of this disease) is characterized by a plurality of malformations that are incompatible with life.
Trisomy is an option aneuploidy , i.e. changes karyotype , in which the human cell has an additional third chromosome instead of normal diploid set.
Monosomy is an option aneuploidy (chromosomal abnormality) in which there are no chromosomes in the chromosome set.
What are the standards for trisomy 13, 18, 21 established during pregnancy? It happens that in the process of cell division a failure occurs. This phenomenon is scientifically called aneuploidy. Trisomy - this is one of the varieties of aneuploidy, in which instead of a pair of chromosomes, an extra third chromosome is present in the cell.
In other words, the child inherits from his parents an additional 13, 18 or 21 chromosome, which in turn entails genetic abnormalities that prevent normal physical and mental development. Down syndrome according to statistics, this is the most common disease due to the presence of chromosome 21.
Children born with Edwards syndrome, the same as in the case of patau syndrome , usually do not live up to a year, unlike those who are not lucky enough to be born with down syndrome . Such people can live to a ripe old age. However, such a life can rather be called existence, especially in the countries of the post-Soviet space, where these people are considered outcasts and they try to avoid and not notice them.
In order to exclude such anomalies, pregnant women, especially those at risk, must undergo a mandatory screening examination. Researchers argue that the development of genetic abnormalities is directly dependent on the age of the expectant mother. The younger the woman, the less likely it is that her child will have any abnormalities.
To establish trisomy in the first trimester of pregnancy, a study is being collar space of the fetus with the help of ultrasound. In the future, pregnant women periodically take a blood test, in which for geneticists the most important indicators are the level alpha-fetoprotein (AFP), inhibin-A, human chorionic gonadotropin (hCG), and estriol .
As mentioned earlier, the risk of having a genetic abnormality in a child depends primarily on the age of the mother. However, there are cases when trisomy is fixed in young women. Therefore, when screening, doctors study all possible signs of anomalies. It is believed that an experienced ultrasound specialist can identify problems during the first screening examination.
Signs of Down syndrome, as well as Edwards and Patau
Trisomy 13 is characterized by a sharp decrease in the level PAPP-A (PAPP associated with pregnancy protein (protein) A-plasma ). Also a marker of this genetic abnormality is. The same parameters play an important role in determining whether the fetus has Edwards syndrome .
When there is no risk of trisomy 18, normal values PAPP-A and b-hCG (free beta subunit of hCG)
recorded in a biochemical blood test. If these values deviate from the standards established for each specific period of pregnancy, then most likely the child will have genetic malformations. 
It is important to note that in the case when, during the first screening, the specialist fixes signs indicating the risk trisomy , the woman is referred for further examination and for a consultation with geneticists. To make a final diagnosis, the expectant mother will have to undergo procedures such as:
- chorion biopsy , i.e. obtaining a sample of chorion tissue for the diagnosis of anomalies;
- amniocentesis- This puncture of the amniotic membrane to get a sample amniotic fluid for the purpose of their further study in the laboratory;
- placentocentesis (biopsy of the placenta) , given invasive diagnostic method specialists take a sample placental tissue using a special puncture needle, which pierces anterior abdominal wall ;
- cordocentesis , a method for diagnosing genetic abnormalities during pregnancy, in which the umbilical cord blood of the fetus is analyzed.
Unfortunately, if a pregnant woman has undergone any of the above studies and is bioscreening and ultrasound the diagnosis of the presence of genetic abnormalities in the fetus has been confirmed, the doctors will offer to terminate the pregnancy. In addition, unlike standard screening studies, data invasive examination methods can provoke a number of serious complications up to spontaneous miscarriage, so doctors resort to them in a fairly rare number of cases.
nasal bone - This is a slightly elongated, quadrangular, convex front paired bone of the human face. At the first ultrasound screening, the specialist determines the length of the baby's nose bone. It is believed that in the presence of genetic abnormalities, this bone develops incorrectly, i.e. its ossification occurs later.

Therefore, if the nasal bone is missing or too small at the first screening, this indicates the possible presence of various anomalies. It is important to emphasize that the length of the nose bone is measured at 13 weeks or at 12 weeks. When screening at 11 weeks, the specialist checks only for its presence.
It is worth emphasizing that if the size of the nasal bone does not correspond to the established norms, but if other basic indicators are consistent, there is really no reason for concern. This state of affairs may be due to the individual characteristics of the development of this particular child.
Heart rate (HR)
A setting such as heart rate plays an important role not only in the early stages, but throughout pregnancy. Constantly measure and monitor fetal heart rate it is necessary only in order to notice deviations in time and, if necessary, save the life of the baby.
Interestingly, although myocardium (heart muscle) begins to decline as early as the third week after conception, you can hear the heartbeat only from the sixth obstetric week. It is believed that at the initial stage of fetal development, the rhythm of its heartbeats should correspond to the mother's pulse (on average, it is 83 beats per minute).
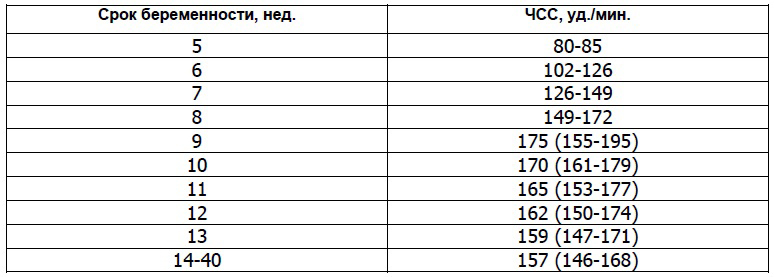
However, already in the first month of intrauterine life, the number of heartbeats of the baby will gradually increase (by about 3 beats per minute every day) and by the ninth week of pregnancy it will reach 175 beats per minute. Determine the fetal heart rate using ultrasound.
During the first ultrasound, specialists pay attention not only to the heart rate, but also to see how the baby's heart develops. To do this, use the so-called four-chamber cut , i.e. method of instrumental diagnosis of malformations of the heart.
It is important to emphasize that the deviation from the standards of such an indicator as heart rate indicates the presence malformations in the development of the heart . Therefore, doctors carefully study the structure on the cut atrial And fetal cardiac ventricles . If any abnormalities are found, the specialists refer the pregnant woman for additional studies, for example, echocardiography (ECG) with dopplerography.
Starting from the twentieth week, the gynecologist of the antenatal clinic will listen to the baby's heart with the power of a special tube at each scheduled visit to the pregnant woman. Such a procedure as auscultation of the heart not applied at earlier dates due to its inefficiency, tk. The doctor just can't hear the heartbeat.
However, as the baby develops, his heart will be heard more and more clearly each time. Auscultation helps the gynecologist determine the position of the fetus in the womb. For example, if the heart is better heard at the level of the mother's navel, then the child is in a transverse position, if the navel is to the left or lower, then the fetus is in cephalic presentation , and if above the navel, then in pelvic .
From the 32nd week of pregnancy, to control the heartbeat, use cardiotocography (abbreviated KTR ). When conducting the above types of examinations, a specialist can record in the fetus:
- bradycardia , i.e. abnormally low heart rate which is usually temporary. This deviation may be a symptom of the mother's autoimmune diseases, anemia, , as well as clamping the umbilical cord, when the unborn child does not receive enough oxygen. The cause of bradycardia can be congenital heart defects in order to exclude or confirm this diagnosis, a woman is necessarily sent for additional examinations;
- , i.e. high heart rate. Such a deviation is rarely recorded by specialists. However, if the heart rate is much higher than prescribed by the norms, then this indicates the mother or hypoxia , development intrauterine infections, anemia and genetic abnormalities at the fetus. In addition, medications a woman takes can affect heart rate.
In addition to the characteristics discussed above, when conducting the first screening ultrasound, specialists also analyze the data:
- about symmetry cerebral hemispheres fetus;
- about the size of the circumference of his head;
- about the distance from the occipital to the frontal bone;
- about the length of the bones of the shoulders, hips and forearms;
- about the structure of the heart;
- about the location and thickness of the chorion (placenta or "baby place");
- about the amount of water (amniotic fluid);
- about the state of the pharynx cervix mothers;
- about the number of vessels in the umbilical cord;
- about the absence or presence uterine hypertonicity .
As a result of ultrasound, in addition to the genetic abnormalities already discussed above ( monosomy or Shereshevsky-Turner syndrome, trisomy on chromosomes 13, 18 and 21 , namely Down, Patau and Edwards syndromes ) the following pathologies in development can be identified:
- neural tube , For example, spinal malformation (meningomyelocele and meningocele) or craniocerebral hernia (encephalocele) ;
- Cornet de Lange syndrome , an anomaly in which multiple malformations are fixed, entailing both physical abnormalities and mental retardation;
- triploidy , a genetic malformation in which a failure occurs in the chromosome set, as a rule, the fetus does not survive in the presence of such a pathology;
- omphalocele , embryonic or umbilical hernia, pathology of the anterior abdominal wall, in which some organs (liver, intestines, and others) develop in a hernial sac outside the abdominal cavity;
- Smith-Opitz syndrome , a genetic deviation that affects the processes, which subsequently leads to the development of many severe pathologies, for example, or mental retardation.
Biochemical screening of the 1st trimester
Let's talk in more detail about the second stage of a comprehensive screening examination of pregnant women. What it is biochemical screening of the 1st trimester, And what are the standards set for its main indicators? In fact, biochemical screening - is nothing but biochemical analysis blood of the expectant mother.
This study is carried out only after ultrasound. This is due to the fact that, thanks to an ultrasound examination, the doctor determines the exact gestational age, on which the standard values of the main indicators of blood biochemistry directly depend. So, remember that you need to go for biochemical screening only with the results of an ultrasound scan.
How to prepare for your first pregnancy screening
We talked about how they do it, and most importantly, when they do a screening ultrasound, now you should pay attention to preparing for the biochemical analysis. As in the case of any other blood test, this study must be prepared in advance.
If you want to get a reliable result of biochemical screening, you will have to follow the following recommendations exactly:
- blood for biochemical screening is taken strictly on an empty stomach, doctors do not even recommend drinking plain water, not to mention any food;
- a few days before the screening, you should change your usual diet and begin to follow a sparing diet, in which you can not eat too fatty and spicy foods (so as not to increase the level), as well as seafood, nuts, chocolate, citrus fruits and other allergenic foods, even if you have not previously had an allergic reaction to anything.
Strict adherence to these recommendations will provide a reliable result of biochemical screening. Believe me, it’s better to be patient for a while and give up your favorite treats so that you don’t worry about the results of the analysis later. After all, any deviation from the established norms, doctors will interpret as a pathology in the development of the baby.
Quite often, in various forums dedicated to pregnancy and childbirth, women talk about how the results of the first screening, expected with such excitement, turned out to be bad, and they were forced to do all the procedures again. Fortunately, in the end, pregnant women received good news about the health of their babies, since the adjusted results showed the absence of any developmental abnormalities. 
The whole point was that expectant mothers were not properly prepared for screening, which ultimately led to inaccurate data.
Imagine how many nerves were spent and bitter tears were shed while women were waiting for new test results.
Such colossal stress does not pass without a trace for the health of any person, and even more so for a pregnant woman.
Biochemical screening of the 1st trimester, interpretation of the results
When conducting the first biochemical screening analysis, indicators such as free β-subunit of human chorionic gonadotropin (Further hCG ), and PAPP-A (plasma protein A associated with pregnancy) . Let's consider each of them in detail.
PAPP-A - what is it?
As mentioned above, PAPP-A - This is an indicator of a biochemical blood test of a pregnant woman, which helps specialists to establish at an early stage the presence of genetic pathologies in the development of the fetus. The full name of this quantity sounds like pregnancy-associated plasma protein A , which in literal translation into Russian means - pregnancy-associated plasma protein A .
It is protein (protein) A, produced during pregnancy by the placenta, that is responsible for the harmonious development of the unborn child. Therefore, an indicator such as the level of PAPP-A, calculated at 12 or 13 weeks during pregnancy, is considered a characteristic marker for determining genetic abnormalities.
It is mandatory to undergo an analysis to check the level of PAPP-A should:
- pregnant women over the age of 35;
- women who have previously given birth to children with genetic abnormalities;
- expectant mothers in whose family there are relatives with genetic abnormalities in development;
- women who have had diseases such as , or shortly before pregnancy;
- pregnant women who have had complications or spontaneous miscarriages in the past.
Normative values of such an indicator as PAPP-A depend on the gestational age. For example, the PAPP-A rate at 12 weeks is 0.79 to 4.76 mU/mL, and at 13 weeks is 1.03 to 6.01 mU/mL. In cases where, as a result of the test, this indicator deviates from the norm, the doctor prescribes additional studies.
If the analysis revealed a low level of PAPP-A, then this may indicate the presence chromosomal abnormalities in child development, for example, down syndrome, Also it signals the risk of spontaneous miscarriage and regressive pregnancy . When this indicator is increased, this is most likely the result of the fact that the doctor could not calculate the correct gestational age.
That is why blood biochemistry is taken only after an ultrasound scan. However, high PAPP-A may also indicate the likelihood of developing genetic abnormalities in the development of the fetus. Therefore, in case of any deviation from the norm, the doctor will refer the woman for an additional examination.
Scientists gave this name to this hormone not by chance, because it is thanks to him that you can reliably find out about pregnancy already 6-8 days after fertilization has occurred. eggs. It is noteworthy that hCG starts to develop chorion already in the first hours of pregnancy.
Moreover, its level is growing rapidly and by the 11-12th week of pregnancy it exceeds the initial values by thousands of times. Then gradually loses its position, and its indicators remain unchanged (starting from the second trimester) until childbirth. All pregnancy test strips contain hCG.

If the level human chorionic gonadotropin increased, this may indicate:
- about the presence of the fetus down syndrome ;
- O multiple pregnancy ;
- about the development of the mother;
When the level of hCG is below the stipulated standards, it says:
- about a possible Edwards syndrome in the fetus;
- about risk miscarriage ;
- O placental insufficiency .
After the pregnant woman has undergone ultrasound and blood biochemistry, the specialist must decipher the results of the examination, as well as calculate the possible risks of developing genetic abnormalities or other pathologies using a special computer program PRISCA (Priska).
The screening summary form will contain the following information:
- about age risk anomalies in development (depending on the age of the pregnant woman, possible deviations change);
- about the values of biochemical parameters of a woman's blood test;
- about the risk of possible diseases;
- MoM coefficient .
In order to calculate as reliably as possible the possible risks of developing certain abnormalities in the fetus, experts calculate the so-called MoM (multiple of median) coefficient. To do this, all the obtained screening data is entered into a program that builds a graph of the deviation of each indicator of the analysis of a particular woman from the average norm established for most pregnant women.
MoM is considered normal if it does not go beyond the range of values from 0.5 to 2.5. At the second stage, this coefficient is adjusted taking into account age, race, presence of diseases (for example, diabetes ), bad habits (for example, smoking), the number of previous pregnancies, ECO and other important factors.
At the final stage, the specialist makes a final conclusion. Remember, only a doctor can correctly interpret screening results. In the video below, the doctor explains all the key points related to the first screening.
1st trimester screening price
The question of how much this study costs and where it is better to take it is of concern to many women. The thing is that not every state clinic can do such a specific examination for free. Based on the reviews left on the forums, many expectant mothers do not trust free medicine at all.
Therefore, you can often meet the question of where to do screening in Moscow or other cities. If we talk about private institutions, then in a fairly well-known and well-established INVITRO laboratory, biochemical screening can be done for 1600 rubles.
True, this cost does not include ultrasound, which the specialist will definitely ask to present before conducting a biochemical analysis. Therefore, you will have to separately undergo an ultrasound examination in another place, and then go to the laboratory for blood donation. And it must be done on the same day.
Second screening during pregnancy, when to do and what is included in the study
According to the recommendations of the World Health Organization (hereinafter referred to as WHO), every woman is required to undergo three screenings throughout the entire period of pregnancy. Although in our time, gynecologists refer all pregnant women to this examination, there are those who, for whatever reason, skip screening.
However, for some categories of women, such a study should be mandatory. This applies primarily to those who have previously given birth to children with genetic abnormalities or malformations. In addition, it is mandatory to undergo screening:
- women over the age of 35, since the risk of developing various pathologies in the fetus depends on the age of the mother;
- women who in the first trimester took drugs or other illegal drugs for pregnant women;
- women who have previously suffered two or more miscarriages;
- women who suffer from one of the following diseases that are inherited to the child - diabetes mellitus, diseases of the musculoskeletal system and the cardiovascular system, and oncopathology;
- women who are at risk of spontaneous miscarriage.
In addition, expectant mothers should definitely undergo screening if they or their spouses were exposed to radiation before conception, and also suffered immediately before or during pregnancy. bacterial and infectious diseases . As with the first screening, the second time, the expectant mother must also do an ultrasound and pass a biochemical blood test, which is often called a triple test.
Timing of the second screening during pregnancy
So, let's answer the question of how many weeks do the second screening
during pregnancy. As we have already determined, the first study is carried out in the early stages of pregnancy, namely in the period from 11 to 13 weeks of the first trimester. The next screening test is carried out during the so-called "golden" period of pregnancy, i.e. in the second trimester, which starts at 14 weeks and ends at 27 weeks. 
The second trimester is called golden because it is during this period of time that all the initial ailments associated with pregnancy ( nausea, weakness, and others) recede, and a woman can fully enjoy her new state, because she feels a powerful surge of strength.
A woman should visit her gynecologist every two weeks so that he can monitor the progress of the pregnancy.
The doctor gives the expectant mother recommendations regarding her interesting situation, and also informs the woman about what examinations and for how long she should undergo. As a standard, a pregnant woman takes a urine test and a complete blood count before each visit to the gynecologist, and the second screening takes place from 16 to 20 weeks of pregnancy.
Ultrasound screening 2nd trimester - what is it?
During the second screening first, an ultrasound scan is performed to determine the exact gestational age, so that later specialists can correctly interpret the results of a biochemical blood test. On ultrasound the doctor studies the development and size of the internal organs of the fetus: the length of the bones, the volume of the chest, head and abdomen, the development of the cerebellum, lungs, brain, spine, heart, bladder, intestines, stomach, eyes, nose, as well as the symmetry of the structure of the face.
In general, everything that is visualized with the help of an ultrasound examination is subjected to analysis. In addition to studying the main characteristics of the development of the baby, experts check:
- how the placenta is located;
- the thickness of the placenta and the degree of its maturity;
- the number of vessels in the umbilical cord;
- condition of the walls, appendages and cervix;
- quantity and quality of amniotic fluid.
Norms for ultrasound screening of the 2nd trimester of pregnancy:
Deciphering the triple test (biochemical blood test)
In the second trimester, experts pay special attention to three markers of genetic abnormalities, such as:
- chorionic gonadotropin - this is produced by the fetal chorion;
- alpha-fetoprotein ( Further AFP ) - This plasma protein (protein), initially produced yellow body, and then produced fetal liver and gastrointestinal tract ;
- free estriol ( further hormone E3 ) is a hormone produced in placenta , and fetal liver.
In some cases, they also study the level inhibin (hormone) produced follicles) . For each week of pregnancy, certain standards are established. It is considered optimal to conduct a triple test at 17 weeks of gestation.
When the level of hCG during the second screening is too high, this may indicate:
- about multiple pregnancy ;
- O diabetes at mother;
- about the risk of developing down syndrome if the other two indicators are below normal.
If hCG, on the contrary, is lowered, then this says:
- about risk Edwards syndrome ;
- O frozen pregnancy;
- O placental insufficiency .
When AFP levels are high, there is a risk of:
- anomalies in development kidney ;
- defects neural tube ;
- developmental disabilities abdominal wall ;
- damage brain ;
- oligohydramnios ;
- fetal death;
- spontaneous miscarriage;
- occurrence Rhesus conflict .
Decreased AFP can be a signal:
- Edwards syndrome ;
- diabetes mothers;
- low location placenta .
At a low level, the risk is high:
- development anemia in the fetus;
- adrenal and placental insufficiency;
- spontaneous miscarriage ;
- availability down syndrome ;
- development intrauterine infection ;
- delays in the physical development of the fetus.
It should be noted that at the level hormone E3 some drugs (for example,), as well as improper and unbalanced nutrition of the mother, affect. When E3 is elevated, doctors diagnose diseases kidney or multiple pregnancy, and also predict preterm birth, when the level of estriol rises sharply.
After the expectant mother goes through two stages of screening, doctors analyze the information received using a special computer program and calculate the same MoM coefficient as in the first study. The conclusion will indicate the risks for a particular type of deviation.
Values are given as a fraction, such as 1:1500 (i.e. one in 1500 pregnancies). It is considered normal if the risk is less than 1:380. Then the conclusion will indicate that the risk is below the cut-off threshold. If the risk is higher than 1:380, then the woman will be referred for additional consultation with geneticists or offered to undergo invasive diagnostics.
It is worth noting that in cases where the biochemical analysis corresponded to the norms during the first screening (indicators were calculated HCG and PAPP-A ), then for the second and third time it is enough for a woman to do only an ultrasound.
The last screening examination of the expectant mother takes place in third trimester . Many people wonder what they look at at the third screening and when this study should be done.
As a rule, if a pregnant woman was not diagnosed with any abnormalities in the development of the fetus or during pregnancy at the first or second examination, then she only has to undergo an ultrasound examination, which will allow the specialist to draw final conclusions about the condition and development of the fetus, as well as his position in the womb. 
Determining the position of the fetus ( head or breech presentation ) is considered an important preparatory stage before childbirth.
In order for the delivery to be successful, and the woman to give birth on her own without surgical intervention, the child must be in the head presentation.
Otherwise, doctors plan a caesarean section.
The third screening includes procedures such as:
- ultrasound , which is passed by all pregnant women without exception;
- dopplerography is a technique that focuses mainly on the condition of the vessels placenta ;
- cardiotocography - a study that allows you to more accurately determine the heart rate of a child in the womb;
- blood biochemistry , during which attention is focused on such markers of genetic and other abnormalities as the level hCG, α-fetoprotein and PAPP-A .
Timing of the third screening during pregnancy
It is worth noting that only the doctor decides how many weeks 3 screening a woman should undergo, based on the individual characteristics of this particular pregnancy. However, it is considered optimal when the expectant mother undergoes a planned ultrasound at 32 weeks, and then immediately passes a biochemical blood test (if indicated), and also undergoes other necessary procedures.
However, for medical reasons, dopplerography or KTG fetus can be from the 28th week of pregnancy. third trimester starts at 28 weeks and ends with childbirth at 40-43 weeks. The last screening ultrasound is usually prescribed at 32-34 weeks.
Deciphering ultrasound
At what time the third screening ultrasound passes a pregnant woman, we found out, now let's talk in more detail about the decoding of the study. When performing an ultrasound in the third trimester, the doctor pays special attention to:
- for the development and construction of cardio-vascular system a child to exclude possible developmental pathologies, for example,;
- for proper development brain , organs of the abdominal cavity, spine and genitourinary system;
- to those in the cranial cavity vein of Galen , which plays an important role in the proper functioning of the brain to eliminate aneurysm ;
- on the structure and development of the face of the child.
In addition, ultrasound allows a specialist to assess the condition amniotic fluid, appendages and uterus mothers, as well as check and placenta thickness . In order to exclude hypoxia and pathologies in the development of the nervous and cardiovascular systems , as well as to identify the features of blood flow in uterine vessels and the child, as well as in the umbilical cord, carry out dopplerography .
As a rule, this procedure is carried out only according to indications simultaneously with ultrasound. In order to exclude fetal hypoxia and define heart rate, carry out KTG . This type of research focuses solely on the functioning of the baby's heart, so cardiotocography prescribed in cases where the doctor has concerns about the condition cardiovascular child systems.
Ultrasound in the third trimester of pregnancy allows you to determine not only the presentation of the child, but also the maturity of his lungs, on which the readiness for birth depends. In some cases, to save the life of the child and the mother, hospitalization may be required for the purpose of early delivery.
| Index | The average rate for 32-34 weeks of pregnancy |
| Placenta thickness | from 25 to 43 mm |
| Amniotic (amniotic) index | 80-280 mm |
| Degree of placental maturity | 1-2 degree of maturation |
| Uterine tone | absent |
| uterine pharynx | closed, length not less than 3 cm |
| Fetal growth | average 45 cm |
| Fetal weight | on average 2 kg |
| Girth of the abdomen of the fetus | 266- 285 mm |
| BDP | 85-89 mm |
| Fetal thigh length | 62-66 mm |
| fetal chest circumference | 309-323 mm |
| Fetal forearm size | 46-55 mm |
| Fetal leg bone size | 52-57 mm |
| Fetal shoulder length | 55-59 mm |
According to the results of a biochemical blood test MoM factor should not deviate from the range from 0.5 to 2.5. The risk value for all possible deviations must correspond to 1:380.
Education: Graduated from Vitebsk State Medical University with a degree in Surgery. At the university, he headed the Council of the Student Scientific Society. Advanced training in 2010 - in the specialty "Oncology" and in 2011 - in the specialty "Mammology, visual forms of oncology".
Experience: Work in the general medical network for 3 years as a surgeon (Vitebsk Emergency Hospital, Liozno Central District Hospital) and part-time as a district oncologist and traumatologist. Work as a pharmaceutical representative for a year in the Rubicon company.
He presented 3 rationalization proposals on the topic “Optimization of antibiotic therapy depending on the species composition of microflora”, 2 works won prizes in the republican competition-review of student scientific works (categories 1 and 3).
The first screening examination is scheduled to detect fetal malformations, analyze the location and blood flow of the placenta, and determine the presence of genetic abnormalities. Ultrasound screening of the 1st trimester is carried out in a period of 10-14 weeks, exclusively as directed by a doctor.
What is a first trimester ultrasound?
Ultrasound is carried out in specially equipped private clinics or antenatal clinics, in which there are appropriate professionals who are able to carry out the necessary diagnostics.
Ultrasound screening of the 1st trimester will help to conduct a full examination at a short period of pregnancy. The attending physician will explain how the study is carried out, and, if necessary, he will tell you how to prepare for the diagnosis.
PAPP-A is a plasma protein A associated with pregnancy. A proportional increase in this indicator indicates the normal course of pregnancy. Deviation from the norm indicates the presence of pathologies in the development of the fetus. However, this only applies to a decrease in the concentration of the indicator in the blood of less than 0.5 MoM; exceeding the norm by more than 2 MoM does not pose any danger to the development of the baby.
Screening of the 1st trimester: deciphering the results of ultrasound and a test for the risk of developing pathologies
Laboratories have special computer programs that, in the presence of individual indicators, calculate the risk of developing chromosomal diseases. Individual metrics include:
- age;
- the presence of bad habits;
- chronic or pathological diseases of the mother.

After entering all the indicators into the program, she will calculate the average PAPP and hCG for a specific gestational age and calculate the risk of developing anomalies. For example, a ratio of 1:200 indicates that a woman out of 200 pregnancies will have 1 child with chromosomal abnormalities, and 199 children will be born completely healthy.
A negative test indicates a low risk of developing Down syndrome in the fetus and does not require any additional tests. The next examination for such a woman will be an ultrasound in
Depending on the ratio obtained in the laboratory, a conclusion is given. It can be positive or negative. A positive test indicates a high degree of probability of having a child with Down syndrome, after which the doctor prescribes additional studies (amniocentesis and chorionic villus biopsy) to make a final diagnosis.
Ultrasound screening of the 1st trimester, reviews of which allow a woman to understand the results more, should not always be taken seriously, because only a doctor can correctly decipher the protocol.
What should be done if there is a high risk of developing Down syndrome?
If you find a high risk of having an unhealthy child, you should not immediately resort to extreme measures to terminate the pregnancy. Initially, it is necessary to visit a geneticist who will conduct all the necessary studies and accurately determine whether there is a risk of the child developing chromosomal abnormalities.
In most cases, genetic examination refutes the presence of problems in the child and therefore the pregnant woman can safely carry and give birth to a child. If the examination confirms the presence of Down syndrome, then the parents must independently decide whether to keep the pregnancy or not.
What indicators can influence the results obtained?
When a woman is fertilized by IVF, the indicators may differ. The concentration of hCG will be exceeded, at the same time PAPP-A will be reduced by approximately 15%, an increase in LZR may be detected on ultrasound.
Weight problems also greatly affect hormone levels. With the development of obesity, the level of hormones increases significantly, but if body weight is excessively low, hormones will also be reduced.

The excitement of the pregnant woman, associated with concerns about the correct development of the fetus, can also affect the results. Therefore, a woman should not set herself up for negativity in advance.
Can a doctor insist on an abortion if Down syndrome is detected in the fetus?
No doctor can force you to terminate a pregnancy. The decision to keep the pregnancy or terminate it can only be made by the parents of the baby. Therefore, it is necessary to carefully consider this issue and determine the pros and cons of having a child with Down syndrome.
Many laboratories allow you to see a three-dimensional picture of a child's development. Photo ultrasound screening of the 1st trimester allows parents to forever keep the memory of the development of their long-awaited baby.
Screening is called research conducted by a complex group of people, in this case, pregnant women at different times. Screening of the first trimester includes ultrasound diagnostics and a biochemical blood test. The study is aimed at identifying possible genetic abnormalities, as well as pathologies of fetal development.
In the first trimester, screening, including a planned ultrasound, is carried out at 11–13 weeks of gestation, which is considered the optimal period for the study. If you do an ultrasound earlier than this period or, conversely, later, then the interpretation of the results may be unreliable.
Of course, a woman can write a refusal to conduct research, even despite the order of the Ministry of Health of the Russian Federation that has been in force since 2000, but such a decision will be extremely risky and even negligent in relation not only to her health, but also to the health of her unborn child.
First trimester screening includes two types of research:
- Ultrasound diagnostics.
- Biochemical study of a blood test.
An ultrasound in the first trimester of pregnancy requires some preparation. To conduct a study in the usual (superficial) way, when the sensor of the device slides over the belly of the expectant mother, her bladder must be full, for which it is necessary to drink about half a liter of pure non-carbonated water 1-1.5 hours before the start of the procedure or 3– 4 hours before the ultrasound, do not urinate.
If the doctor will do the procedure in a transvaginal way, when a special sensor of the device is inserted into the vagina, then special preparation is not required. The pregnant woman must go to the toilet before starting the procedure.
A biochemical blood test is the second stage of screening and is carried out only after ultrasound. This condition is important, since the obtained indicators always depend on the gestational age and change every day, and the exact period can only be established with the help of ultrasound. This condition must be observed in order to obtain the correct interpretation of the study indicators and establish compliance with the necessary standards.
At the time of blood sampling for analysis, the woman should have the results of the first part of the study ready, where the exact gestational age will be indicated. If the ultrasound test procedure showed the regression of pregnancy or its fading, then there is no point in conducting the second part of the screening.
A biochemical study requires preparation so that the doctor can obtain accurate indicators and determine their compliance with the standards. Blood sampling from a vein is carried out strictly on an empty stomach.
Approximately 2-3 days before visiting the treatment room, it is necessary: to exclude from the diet sweets, smoked meats, fried and fatty foods, as well as foods that are potential allergens, such as nuts, chocolate, citrus fruits, seafood.
Failure to comply with these conditions often leads to inaccurate research results.
What can be learned from screening?
In order for the decoding of ultrasound to be reliable and informative, it is necessary to carry out the procedure no earlier than 11 weeks of pregnancy, but no later than 13.
The position of the fetus should be convenient for inspection and measurement. If the position of the child does not allow for an ultrasound procedure, the woman is asked to turn on her side, walk around, do a few squats or cough so that the baby rolls over.

Indicators that should be investigated during the ultrasound in the first third of pregnancy:
- Coccyx-parietal size (KTR). The measurement is taken from the parietal point of the head to the coccyx.
- Biparietal size (BDP) is the distance between the tubercles of the parietal zone.
- Head circumference.
- The distance from the back of the head to the frontal zone.
- The structure of the brain, the symmetry of the location of the hemispheres, the closure of the cranium.
- The thickness of the collar zone (TVP).
- Heart rate (HR).
- The size of the heart, as well as the largest vessels.
- The length of the bones of the shoulders, thighs, lower leg and forearm.
- The thickness of the placenta, its structure and location in the uterus.
- The location of the umbilical cord and the number of vessels in it.
- Volume of amniotic fluid.
- Tone of the uterus.
- Condition of the cervix and its internal os.
When an ultrasound is performed ahead of schedule, the doctor cannot assess the size of the nasal bone, the CTE of the fetus is from 33 to 41 mm, which is not enough to conduct an adequate study. Heart rate during this period ranges from 161 to 179 beats, TP from 1.5 to 2.2 mm, and BDP is 14 mm.
The norms for decoding indicators for this period:
- At 11 weeks, the nasal bone of the fetus is visible, but its dimensions cannot always be estimated. The KTR of the crumbs is from 42 to 50 mm, the BDP is 17 mm, the TVP is from 1.6 to 2.4 mm, and the heart rate is from 153 to 177 beats.
- At 12 weeks, the size of the nasal bone is 3 mm or slightly more. CTE is in the range of 51-59 mm, BDP is 20 mm, TBP is from 1.6 to 2.5 mm, and heart rate is from 150 to 174.
- At 13 weeks, the size of the nasal bone is more than 3 mm. CTE is in the range from 62 to 73 mm, BDP is 26 mm, TBP is from 1.7 to 2.7, and heart rate is from 147 to 171 beats per minute.
During biochemical screening, a number of important indicators are determined, one of which is the chorionic gonadotropin β-hCG produced by the fetal membrane. It is this hormone that allows you to determine the presence of pregnancy at the earliest possible time when using a special test strip.
From the beginning of pregnancy, during its normal course, the level of β-hCG gradually increases, reaching a maximum value by week 12, after which it decreases. During the second half of the term, the indicators of β-hCG remain at the same level.
The norm of indicators of β-hCG is:
- Week 10: 25.80 to 181.60 ng/mL;
- 11 weeks from 17.4 to 130.3 ng / ml;
- 12 weeks from 13.4 to 128.5 ng / ml;
- 13 weeks from 14.2 to 114.8 ng / ml.
Elevated values are observed with Down's syndrome in a developing fetus or when the expectant mother has a severe form of toxicosis, as well as diabetes mellitus.
Decreased rates may indicate placental insufficiency (which is usually established during an ultrasound scan) or that the fetus has Edwards syndrome.
The second important indicator is protein-A (PAPP-A), which is associated with pregnancy, since this protein is produced by the placenta and is responsible for its proper functioning and development.

The following data are considered normal indicators of PAPP-A:
- From 10 to 11 weeks from 0.45 to 3.73 mU / ml;
- From 11 to 12 weeks from 0.78 to 4.77 mU / ml;
- From 12 to 13 weeks from 1.03 to 6.02 mU / ml;
- From 13 to 14 weeks from 1.47 to 8.55 mU / ml.
If the indicators are below the norm, this may indicate not only the threat of a miscarriage, but also the presence of Edwards, Down or Cornelia de Lange syndrome in the fetus. In some cases, there is an increase in protein levels, but this does not have significant diagnostic and clinical significance.
MoM coefficient calculation
The calculation of this indicator is done according to the results of the research. Its value indicates the degree of deviation of the test results from the established average norms, which range from 0.5 to 2.5 for singleton pregnancies and up to 3.5 for multiple pregnancies.
In different laboratories, when examining the same blood sample, the indicators may differ, therefore, it is impossible to evaluate the results on your own, only a doctor can do this.

When deriving the coefficient, not only tests are necessarily taken into account, but also the age of the expectant mother, the presence of chronic diseases, diabetes, bad habits, the weight of the pregnant woman, the number of fetuses developing inside, and also how the pregnancy occurred (naturally or with the help of IVF). The risk of developing pathologies in the fetus is considered high at a ratio below 1:380.
It is important to correctly understand the meaning of this ratio. For example, if the conclusion says "1:290, high risk," this means that in 290 women with the same data, only one child had a genetic pathology.
There are situations when averages deviate from the norm for other reasons, for example:
- if a woman is overweight or severely obese, hormone levels are often elevated;
- with IVF, PAPP-A indicators will be below the general average, and β-hCG, on the contrary, will be higher;
- an increase in the normal level of hormones can also be observed when the expectant mother has diabetes;
- for multiple pregnancies, average norms have not been established, but the level of β-hCG is always higher than with the development of a single fetus.
Conducting research in the first trimester allows you to establish the presence (absence) of many pathologies in the developing fetus, for example:
- Meningocele and its varieties (pathologies of neural tube development).
- Down Syndrome. Trisomy 21 occurs in one case out of 700 examinations, but due to timely diagnosis, the birth of sick babies has decreased to 1 in 1100 cases.
- Omphalocele. With this pathology, a hernial sac is formed on the anterior abdominal wall of the fetus, into which part of the internal organs enters.
- Edwards syndrome, which is a trisomy of chromosome 18. Occurs in one in 7,000 cases. It is more common in babies whose mothers are over 35 years old at the time of pregnancy. During ultrasound, the fetus has an omphalocele, a decrease in heart rate, and the bones of the nose are not visible. In addition, violations of the structure of the umbilical cord are also detected, in which instead of two arteries there is only one.
- Patau syndrome, which is a trisomy of chromosome 13. It is very rare, on the order of one in 10,000 newborns, and typically about 95% of infants with this syndrome die within the first months of life. When conducting ultrasound in these cases, the doctor notes slowdowns in the development of tubular bones and the brain, omphalocele and increased heart rate in the fetus.
- Triploidy, which is a genetic anomaly characterized by a triple set of chromosomes, which is accompanied by the occurrence of many developmental disorders.
- Smith-Opitz syndrome. The disorder is an autosomal recessive genetic disorder in which metabolic disorders occur. As a result, the developing fetus has many defects and pathologies, autism, and mental retardation. The syndrome occurs in one case out of 30,000.
- Cornelia de Lange syndrome, which is a genetic anomaly that causes mental retardation in an unborn child. Occurs in one case out of 10,000.
- Fetal anencephaly. This developmental pathology is rare. Babies with this disorder can develop inside the womb, but they are unable to live and die immediately after birth or while in the womb at a later date. With this anomaly, the fetus is missing the brain and bones of the cranial vault.
Screening in the first trimester can detect many chromosomal diseases and developmental disorders in the unborn child in early pregnancy. Screening allows you to reduce the percentage of babies born with congenital anomalies, as well as save many pregnancies in which there is a threat of termination, by taking timely measures.







